

NOTICE:
This document is currently under construction.
AND, I attempted to Condense an Intensive, Two Day Workshop
into this paper. … So there’s a LOT here already!
| Having had experience with many different bodyworkers, David’s technique is certainly unique. There are levels of healing he achieves I’ve never seen before. This is clearly a result of a vast knowledge of anatomy and physiology combined with decades of hands-on experience. Dr. John Bordiuk • Internist, Nutritional M.D. Inner Balance Med • Wellesley, MA |
I have worked with many soft tissue therapists over the years. David Scott Lynn is the only one educated and skilled enough to do what I want with full confidence that the job will be done. My patients definitely feel the difference. Gary Fujinami • Doctor of Chiropractic East West Chiropractic & Acupuncture Center Prescott, Arizona |
— DSL EdgeWork & Let-Go Yoga —
The DSL Method
An Integrated System of Physical/Mental Yoga;
BIO-Structural, Hands-On BodyWork & Principles of Natural Healing,
Based on a Wholistic Foundation of a Philosophy, Psychology
& Sciences of Being Human
Developed & Presented by David Scott Lynn (DSL)
PERSONAL NOTE: There is in the soft-tissue world a multitude of widely available and very effective therapies. I know and assume many are valid & effective modalities and healing philosophies, and I do not intend to imply that what I do is necessarily superior, in any general sense, to any other methods.
That said, there are certain Client challenges appearing almost uniquely responsive to the specific manual techniques the DSL Method utilizes, with its several important nuances. Although effective for most people, Clients I’ve worked with tend to be otherwise less- or un-responsive to many or most other modalities, or the technique works, but the client must return periodically as the symptoms perpetually return. And many have literally spent years or even decades looking for relief, trying many orthodox and alternative therapies that would solve their problems of pain and/or dysfunction, yet to no avail.
It is my assessment that of the total Patient Population, probably only less than 5% actually need the detail the DSL Method goes into to get people better. But when that specific process is what you need, then that’s what you need. And that’s what I, founder of the DSL Method, provide … that specific process.
On the other hand, the dynamics behind what I do & teach also serve to inform everyone of certain Principles & Practices that appear to be universal to every human being, and can be applied to nearly every system of therapy. Therein lie the preventive & maintenance principles & practices universal to us all, and to al healing modalities. …
Hopefully, you will find these principles useful in many ways.
Thank You Very Much for Taking the Time to Read This,
David Scott Lynn
C.E.M.&.N.T. (Chronic, Excess Muscle & Nerve Tension)
Dr. John Bonica, a forerunner in modern management of soft tissue pain and injury and early advocate of Trigger Point Therapy, said in his 1,700 page, two volume book The Management of Pain, that soft tissue injuries were the most common form of injury in America:
In the United States and most industrialized nations, disorders of muscles, tendons, fascia, bones, joints and their ligaments are the most frequent cause of pain, disability, limitation of activity and impairment. … the most frequent cause of chronic or permanent impairment.
John J. Bonica, M.D.
The Management of Pain
2nd Edition; page 328
What Dr. Bonica is indirectly referring to, of course, is in great part resultant from excess nerve & muscle tension and stress, what we are here calling C.E.M.&.N.T. (Chronic, Excess Muscle & Nerve Tension) …
What causes C.E.M.&.N.T. is the most common question from students, clients and patients alike, as well as health care professionals seeking more knowledge on how to work with these issues. Yet like many things, when you know what it is and how it works, you often spontaneously see the solutions to the problems.
The Primary Goal of this Summary is to Provide Physicians & Therapists with:
1.) Enough knowledge to understand what the C.E.M.&.N.T. approach is all about.
2.) A basis to begin adding the potential diagnosis of C.E.M.&.N.T. into their evaluations of Patients.
3.) Ability to direct one or more hands-on and/or “stretching” therapists in administration of appropriate manual techniques for resolution of C.E.M.&.N.T.
4.) How to effectively recommend proper self-care techniques to Patients after treatment (and use them for the practitioners’ own selves, as well).
SAMPLE of Case Studies Utilizing DSL Edgework (Upper Limb)
Clinical Bias & Target Clientele:
The Bias in this Perspective & Results lie in in the following:
Clients or Patients who can benefit tend to be People who:
1.) Have been to many physicians & practitioners of a wide range of modalities with little or no results, or intermittently beneficial, but not long lasting. (They are often close to “giving up.”)
2.) Have very little or no indication of pathology on X-Ray or MRI, or if they do, it is difficult to make a direct and strong correlation between visible pathology (such as so-called arthritic deposits, or herniated discs) and the presenting pain or dysfunction. (And it is becoming more widely known that such “structural” elements of deteriorating bones, joints, cartilage, etc., are NOT really the cause of pain or dysfunction. Much or most of it is actually in the soft tissues and neural or mental / emotional structures.)
3.) Have problems reasonably consistent with neuromuscular & myofascial (soft tissue) issues, sometimes but not necessarily with a psychological component. (It is sometimes difficult to distinguish between pain from physical causes versus pain from emotional causes.) I believe most musculoskeletal issues are indeed resultant from neuromuscular & myofascial causes, including much of joint degeneration.
4.) Present with symptoms consistent with Chronic, Excess Muscle & Nerve Tension (C.E.M.&.N.T.). Yet it is usually vastly understated as to how many health issues are potentially the result of C.E.M.&.N.T.
NOTE: C.E.M.&.N.T. is a term comparable to the terms MPS (myofascial pain syndrome), and/or TMS (Tension Myositis Syndrome). I will discuss these terms on another page of this website.
Determining which conditions, syndromes & symptoms are consistent with C.E.M.&.N.T. is not always easy, as they can be quite pervasive (i.e., some people feel “tight all over” and function as such). C.E.M.&.N.T. is often surprising in its range of potential secondary effects and resulting symptoms. But when all other modalities, including metabolic, are not working, chronic muscle tension is often all that is left. And, muscle being such a high percentage of tissue in the body, and with its level of fragility (event though powerful), increasing amounts of research point to chronic muscle or (sometimes) “trigger point” issues as a primary cause of much pain & dysfunction. (It is the fascial sheaths of each muscle fiber and fiber groups providing the “toughness” of apparent muscles.)
Structural Evaluation Principles:
In structural analysis, including postural evaluation, there are, generally speaking, five classifications of structural imbalance generated by C.E.M.&.N.T.:
- Localized Stress, Tension & Trauma
- Generalized Musculoskeletal Compression
- Structurally Transmitted Strains & Asymmetries
- Neuralgic Stress & Transmissions
- Antalgic Reactions
These will be described & discussed later in this Summary.
The manual techniques employed by DSL’s methods have an added benefit of being among the least invasive measures available, yet with a high degree of healing power. It should be noted, however, that the primary source of “healing power” is thought to be by way of stimulating the bodies own natural self-healing methods, by way of stimulating (primarily) the parasympathetic nervous system. Stress and tension tend to activate the sympathetic system while diminishing parasympathetic function. Our primary intent is to reverse that process.
Fundamental Principles of DSL EdgeWork
The Condition of C.E.M.&.N.T. … or Chronic, Excess Muscle & Nerve Tension:
NOTE: Upon reflection, the term should actually be Chronic, Excess Muscle & Nerve Tension & Stress. However the acronym — C.E.M.&.N.T.S. — would tend to get out of hand. So I stayed with the less complete term.
What Is C.E.M.&.N.T. ?
As per the Law of Facilitation* (or Law of Habit, or synaptic plasticity), repetitive firing of nerve pathways increases the firing of said pathways, and all muscles, glands & organs receiving stimulus from said pathway will be in an increasingly stimulated or eventually irritated state.
Law of Facilitation: When an impulse has passed once through a certain set of neurons to the exclusion of others, it will tend to take the same course on a future occasion, and each time it traverses this path the resistance in the path will be smaller.
Dorland’s Medical Dictionary, 25th Edition
In addition, any neural pathways firing simultaneously along with other pathways will tend to develop habitual synaptic associations tending to fire together.
“What fires together, wires together.” … Hebbian Theory of Learning
~Introduced by Donald Hebb in his 1949 book The Organization of Behavior
ANY activation of the nervous system, with any degree of frequency, and even if minimal to moderate force, would tend to bring the law of facilitation (or synaptic plasticity) into play. Be it mental, emotional or physical, if it utilizes the nervous system for its function, including memory & thinking (meaning just about everything), are in one way functions of synaptic facilitation. Therefore, nearly any activity, if a nerve is involved, is subject to, or a product of, this facilitation. As nerve activity is increased, all muscles, organs or systems on that nerve pathway will be stimulated.
The more frequent, or the stronger the contraction, the more synapses are recruited, and the more pathways are facilitated. When injury or trauma occurs, multiple pathways are instantly recruited to engage protective and stabilizing forces within the body. So, while walking facilitates pathways, a run facilitates far more, and falling down on the sidewalk even more.
Accumulated tension & stress from walking and running are more a function of temporal facilitation, the stimulation of synapses repeatedly over time. The falling down, or a car accident and such, is more a product of spatial facilitation, where multiple pathways are simultaneously facilitated in an instant, or very short period of time.
The original and repetitive stimulation eventually becomes habitual or chronic, and from that point on, nerves, muscles and/or organs never get an opportunity to fully Relax, Rest & Rejuvenate (3-Rs). Therefore, Resting Tonus increases. As resting tonus increases, the strength and intensity of chronic muscle contraction increases, and the muscle increasingly shortens, or attempts to. The more a muscle attempts to shorten, but it’s corresponding bone does not move (because of counter-forces by opposing muscles, gravitational issues or other exogenous pressures), then increasing stress is applied to the muscle cells, fascial sheaths & tendons, and periosteum.
Resting Tonus: Chronically accumulated nerve charge keeping muscle cells in a continuously activated state. This activation shows up, in part, as chronic muscle contraction, and tendency toward shortening. That in turn shows up, eventually, as slowed reflexes & response time.
The Fitness Factor
It is ironic that among my Clients, the ones who are most “physically fit” are often the ones with the most neuro-musculo-fascial problems (aches, pains, dysfunction). This is in great part because they’ve invested so much energy & time in engaging large numbers of neuro-musculo-skeletal pathways & synapses to achieve the desired actions within their fitness activities. They also are engaging more fully the alpha pathways, not just the gamma pathways, so there is more participation from higher levels of the nervous system and brain.
Neuromuscular *Discombobulation*
Finally, because of more frequent, higher intensity activity, there is more likelihood of “neuro-musculo-fascial discombobulation” — literally, a confusion or dis-coordination of adjacent or nearby neuromuscular sensory-motor units when a body part encounters some anomaly divergent from normal movement patterns. This distorts the otherwise smooth function of the actin-myosin units (sarcomeres), and sensory-motor feedback loops creating a *Garbage In, Garbage Out* type of effect computer programmers encounter when computer code values are distorted or corrupted.
It is important to note that a “tight muscle” by itself, or poor posture by itself, or a somewhat faulty gait by itself, are seldom sufficient to cause a pain or dysfunction pattern. I believe it requires multiple factors, or another factor all together. Discombobulation (literally, to disconcert or to confuse) might very well be that factor in many cases.
Chronic Over-shortening of Muscles can:
1.) apply pressure on many different tissue structures in the area of over-shortened muscles such as nerves, blood vessels and organs.
2.) apply tensions to the bone structures, therefore distorting posture, in turn requiring compensations by other muscles at other points in the structure. Wolf’s Law also states that bony deposits will form as pressures are increased on the bone by muscular force. This leads to build ups such as so-called “arthritic deposits,” actually enthesophyte deposits of bone at the tendon and ligament attachments. It is hypothesized that the constant pressures of ones pulling on their attachments initiating formation of excess bony deposits or “bone spurs.”
3.) apply pressures across joint structures, compressing said joints, dehydrating them, reducing synovial fluid and lubrication. This eventually increases pressure on joint surfaces and cartilage with eventual erosion and degeneration.
4.) reduce range of motion of respective body segments.
5.) reduce ability to lengthen or shorten in coordinated function.
One important element of a chronically over-shortened muscle that might or might not be obvious is it cannot lengthen out instantaneously as can a normal muscle. This reduced ability, however slight, to instantly adjust length appropriately is an important factor in balance and coordination, as well as overall speed of movement. If its antagonist is equally tight, shortening of the muscle fiber is also impaired. Reduced ability to instantly respond to neural inputs impairs coordination, agility and balance.
6.) reduce local metabolic function.
Metabolic processes are therefore interfered with (such as constriction of blood vessels and restriction of lymphatic detoxification), in that incoming nutrients are inhibited and tissue detoxification becomes less efficient. As well, research shows chronic tension being responsible for the build up of various chemical constituents:
“… a biochemical milieu of selected inflammatory mediators, neuropeptides, cytokines, and catecholamines …”
Archives of Physical Medicine & Rehabilitation
2008, Volume 89, Number 1, Pages 16–23
http://www.ncbi.nlm.nih.gov/pubmed/18164325
7.) apply excessive contractile forces on to usually synergistic muscles, turning synergists into antagonists.
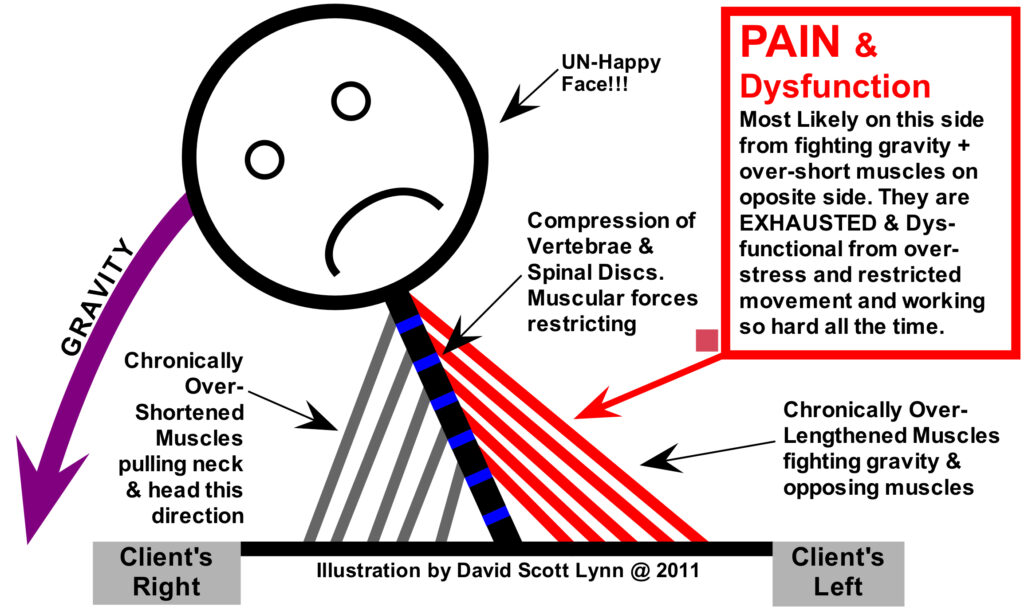
The antagonists tend to be over-lengthened, which in many cases causes them to be even more compromised than the over-short muscles. They often actually feel and function as if they are “tighter” than the over-shortened opposing muscles, which they often actually are. (Discussed and illustrated further below.) Over-lengthened muscles tend to be the more painful and show up as “weak” when in actuality, they are NOT fundamentally weak, but exhausted and deprived of mechanical advantage.
(Often mistaken for fundamental “weakness,” over-shortened muscles are termed actively insufficient and show up as “weak.” Over-lengthened muscles are passively insufficient also presenting as “weak.” However, in many cases, this is really what I call pseudo-weakness. The weakness is functional, not fundamental.
8.) Additionally, muscular forces on various hard and soft tissues increases general stress and wear & tear, therefore causing significant breakdowns in all such tissues. With these multiple factors accumulating in the background of the human structure and tissues, various forms of deterioration eventually set in.
For One Example: Originating at T-12, the psoas muscles traverses all the vertebrae of the lumbar spine. As it chronically shortens, the available space for the discs diminishes, compressing the discs, eventually breaking down the tissues to varying degrees. This leads to all kinds of secondary problems.
This principle of joint compression applies to any joint of the body. We now have a better explanation than “you’re just getting old” when a disc or joint capsule starts to degenerate and eventually break down.
Further Note on Psoas: There is a little known, deepest layer of psoas major, named Pars Vertebralis, adding a level of compression to the dynamics of psoas. These fibers traverse from vertebral body to body, but do not continue downward beyond the spinal column. Their contractive forces proximate the vertebral bodies, directly compressing the discs.
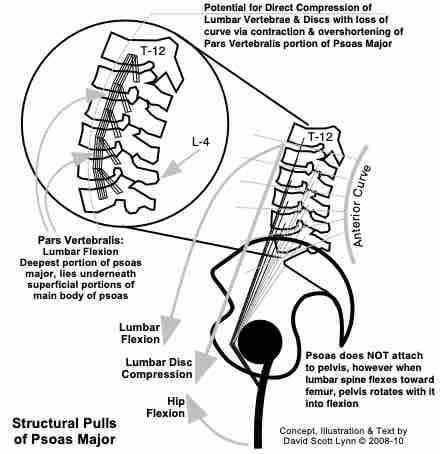
Normal Psoas Muscle with Pars Vertebralis
Please See my BodyMind Breakdowns Min-e-Course (or e-book) for more details.
Where & How Does C.E.M.&.N.T. Originate?
As stated above, any activity firing a synapse and nerve pathway frequently enough, with enough force, will facilitate the pathway. The amount of force does not need to be much. In fact … Gentle walking, or typing, or playing a musical instrument will all do it. Yet everyone is different. The rate at which C.E.M.&.N.T. accumulates is different for all of us. And so too, the rate at which varying amounts of C.E.M.&.N.T. will become a problem for any particular individual, compared to others, varies greatly.
Just sitting slouched on a couch can generate chronic neuromuscular facilitation. Many people would assume the belly muscles go flaccid when sitting in a couch or chair with little or no lumbar support. Yet the abdominal wall muscles are indeed contracting, becoming chronically so over enough time spent slouched on that couch.
According to Davis’ Law, when the two ends of a muscle are brought towards each other, the tonus within that muscle must increase to take up the slack in that muscle. This is necessary otherwise any muscle powered entity would move like a rag doll much of the time. So, if your patient is sitting in a couch with rib cage proximated toward the pelvis (very common), then the span between ribs and pelvis must be shorter. This produces slack in the abdominal wall muscles. The nervous system, by way of reduced stimulation to the Golgi Tendon Organs, will automatically and instantly take up that slack by shortening the slackened muscles.
This is achieved via the intrafusal muscle fibers. While only approximately 30% of a muscle’s mass on average, they have striated, contractile muscle fibers. They might not be strong enough to accomplish significant amounts of action with strength, but they can reset the resting tonus and overall habitual length of a muscle. Controlled by the gamma system they are not under direct conscious control, yet the alpha system can influence the gamma system to some degree.
I have my own doubts about orthodox allegations that intrafusal fibers are not capable of exerting at least some degree of pathological forces onto body structures. They might not create significant action, but I strongly speculate they are strong enough to, for example, resist the bone structure moving upward to more vertical, balanced posture. Or they keep bones & joints from moving quickly and easily.
This is why, for example, a person who holds their shoulders up all the time can, when you point it out to them, put their shoulders down. Yet a few minutes later, they are back up again. They engaged their alpha system that inhibits the gamma controlled intrafusal shortening, so the muscles can lengthen out and return to “normal.” But as soon as they move their conscious attention to something else, the alpha system is no longer engaged in that area, and the gamma system takes control again, re-establishing the historical & habitual contractions of the gamma-controlled, intrafusal fibers.
IMPORTANT NOTE: Due to a little reported flaw in EMG equipment, I believe many errors were made in the 1970s – 80s while assessing strength & weakness, activity & passivity, in muscle fibers. EMG devices were able to measure the output of the extrafusal muscle fibers. But the activity of the intrafusal fibers remained silent to the machinery. They could not reliably determine whether the intrafusal fibers were active or not. Therefore, I think it quite likely that muscles that were indeed active by way of intrafusal activity, though not a very strong force, had an important yet unrealized affect on posture and movement.
This discovery and realization caused a neurologist (licensed M.D.), who had been treating paralytic patients for over 25 years in Duluth, Minnesota, to tell me that based on what she had learned from me in workshops, and observed in our results with patients, that the medical profession had been treating paralytic patients backwards for at least the 25 years he had been practicing. This included Parkinson’s and MS patients.
Because the EMGs had been reporting lack of activity or “weakness” in the muscles, therapy had been geared toward activating the neuromuscular units with “strengthening” types of exercise. Yet the RAS (reticular activating system, working via the gamma and intrafusal system) might have been VERY active, yet exhausted.
Excess activation of the descending sensory pathways would also interfere with proper sensory-motor feedback loops, potentially interfering with the ability of the alpha-extrafusal system to function. Combined with active & passive insufficiency in pairs of out-of-balance muscles, it is no wonder their systems were shutting down.
Resting Tonus
At one level, and the simplest, C.E.M.&.N.T. is just the process of life itself bringing on accumulations of Chronic, Excess Muscle & Nerve Tension. Any repetitive action, done often enough, and with enough force (and surprisingly small amounts of force), will initiate increasing facilitation of neuromuscular pathways, in turn raising the Resting Tonus of the neuro-musculo-fascial system.
The unfortunate result of increasing Resting Tonus throughout life is the anti-postural muscles become increasingly more contracted and over-shortened, gradually decreasing their potential response time. Some opposing “postural” muscles actually get over-lengthened, yet they, paradoxically, often end up “tighter,” more painful, and dysfunctional than their over-shortened synergists. This is due to gravitational and postural forces putting more stress on the over-lengthened muscles.
Accumulation of Resting Tonus is much of what produces the feeling of getting “tighter” over the years, with less responsive muscles, and decreased balance and coordination. Just going for regular, long walks increases (though mildly) facilitation of all involved nerves and muscles, quietly increasing Resting Tonus in the background, usually unnoticed for years or decades. The greater intensity and frequency of ANY exercise involves heightened levels of contractile response with this nearly unavoidable reality.
There is literally NO fitness oriented (SECC — Strength, Endurance, Cardio & Coordination) exercise that completely avoids such accumulations of C.E.M.&.N.T. This is one reason we believe there is no one “balanced” exercise. We need at least one exercise that activates SECC, and another that DE-activates the inevitable C.E.M.&.N.T.
Some people pretend things like Power Yoga are a good balance between strengthening and relaxation. Unfortunately, most “power”-type Yoga classes have the student, and the teacher (!) in too high of a sympathetic, tension building state, increasing C.E.M.&.N.T., and usually not even knowing it. Yet they are often, paradoxically, getting more flexible, and believe that increasing flexibility indicates they are getting more “relaxed” or even “healthier.”
Therein lies a Paradox: that one can get more flexible, yet still have their muscles be “tighter” and actually LESS fundamentally relaxed. (Explaining that would go WAY beyond the scope of this Summary.)
Beyond the contractions of discrete neuromuscular units, though, various stresses in the connective tissues — muscle sheaths, tendons, ligaments and periosteum — will, from different physiological mechanisms, build up as well. Connective tissue — also know as fascia* — has primarily sensory, and very little, if any, motor enervation. Negative accumulations in fascia are in my view more biochemical, metabolic and structural in nature, rather than directly motor induced. However, due to significant sensory innervation in connective tissues (fascia), too many biochemical and structural stresses building up can certainly stimulate heightened sensory input to the CNS, in turn activating motor irritation reactivity.
Fascia: The 37th Edition of Grays’s Anatomy (the Really Big & Expensive one from Elsevier, not the original one can you get in many bookstores for ten bucks) said the word fascia had become so over-used as to have become nearly meaningless. The Fad of Fascia and it’s many “profound” implications, has indeed been far overdone, with certain properties attributed to it that defy scientific rationale. This is why we prefer to refer to the musculo-fascial unit, indicating that the muscle and fascia work together, and are treated and exercised, as a fully integrated unit. There is little that can be done with fascia independently from the muscle fibers, and vice versa.
Please see my further discussion of fascia here: What Ever Happened to the Myo in Myofascial Release?
Magnification from Injury
Any sudden events such as accidents, trauma or other injuries accelerate the C.E.M.&.N.T. accumulation process, sometimes dramatically and instantaneously. The degree of intensity of the event is often multiplied by the nervous system response. The earlier mentioned difference between temporal and spatial synaptic facilitation are important concepts here.
Thixotropy
Another important factor in connective tissue is thixotropy, or, in laymen’s language, “gluing” of soft tissues. For example, one substance, hyaluronic acid, is in normal conditions a lubricant within and between body tissues. When its energy levels decrease, however, it moves from a more fluid, lubricating state (a sol) to a more dense, “sticky” state (gel). At the extreme, the “stickiness” can eventually create such tight chemical bonds they cannot be broken, similar to when scar tissue (cross-linking of colloidal molecules) forms.
Now, it is very possible that this “gluing” (thixotropic) phenomena has, along with the Fad of Fascia, been very overstated, especially when manual therapists start talking about “adhesions.” While theoretically quite possible, it has been my experience that many of those “tight spots” in tissue, areas assessed by others as “adhesions” (thixotropic), were actually just extremely contracted muscle fibers.
And rather than “breaking up adhesions,” what was really necessary is the overly tight muscles needed relaxation (DE-contraction). (It is quite amazing how tight, even sharp, some of these contracted nodules can feel. So it’s no surprise less manually dextrous therapists will make this incorrect assessment.) There might well have been some degree of stickiness or adhesion going on, but it was minor compared to the affect of the C.E.M.&.N.T. itself.
Thankfully, regardless of the truth of all that, if pursued soon enough, adding kinetic energy of any kind, without getting too aggressive and triggering defense mechanisms, can help move such fluids back from the sticky to the lubricating state without too much effort. … Just one more reason exercises like gentle yoga and tai chi and even Swedish style massage done as preventive maintenance from early adulthood or even childhood can be very long-term beneficial.
(Hyaluronic acid also binds significant amounts of water in the soft tissues. DSL Edgework puts much focus on the function of water in human structure & function, such as it’s protective function. Many problems appear to actually be caused by chronic dehydration. We’ll briefly address this later in this paper.
A great resource, however, is Dr. Batmanghelidj, author of Your Bodies Many Cries for Water, and You’re Not Sick, You’re Thirsty. His perspectives are controversial, but very well developed in his books. Like most things in alternative medicine, it would be great if funds were made available to actually do studies to test such theories.)
Warming Up & Thermal Expansion: A Fitness & Flexibility Illusion
One complicating factor producing certain illusions is that much of what we do to initiate neuromuscular facilitation (walking, running, exercise) also “warms up” the same tissues at the same time. So, the warmed up tissues feel in that moment and soon after as “looser.” Yet this is at the purely structural level, and they probably are “looser,” due to increased “molecular heat” or the well-known physics of thermal expansion.
This is the same reason telephone wires hang lower in summer time than they do in winter. The faster molecules move from increased heat, the more space they take up (thermal expansion), causing an increase in the volume of the tissue or substance in question. So too, as muscles heat up, they expand, get longer, and put less pressure on surrounding tissues. Therefore, you feel looser and in many ways, and less stressed. That’s because physical, outward expressions or manifestations of stress are reduced, even if the internal source or root cause of such stress is not addressed or resolved. So, for example, running can help one “blow off steam” even though it does nothing to help the actual situation causing internal stress in the first place.
The short-term perception, then, is “walking (or running, or whatever) loosens you up.” Yet in the background, increased neuromuscular facilitation is slowly increasing the Resting Tonus of the involved units. How that shows up is, over the years, when the same person wakes up in the morning, after several hours of sleeping and their muscles cooling down (thermal contraction), they feel tighter, more “creaky,” more achy or even in varying degrees of pain. It’s like a race between keeping my muscles “warmed up” enough to stay ahead of my accumulating C.E.M.&.N.T.
More aggressive exercise like running or power yoga produces similar effects, although the psycho-neuro-muscular facilitation levels are much higher than with relatively relaxed walking. (On the positive side, this kinetic warming up can also help prevent or reduce the above mentioned thixotropy by keeping everything moving, and kinetic energy levels higher.)
Sherrington’s law of Reciprocal Innervation, also called Sherrington’s Law, II
Some clinicians object that the function of Reciprocal Innervation (RI) handles much of the problem of C.E.M.&.N.T. The theory is when one muscle contracts, the opposite muscle is equally DE-contracted by inhibition via the spinal cord reflexes. This is true, up to a point. However, when Resting Tonus has developed beyond a certain level (not a specifically quantifiable level, and different for everyone) then it interferes with the smooth functioning of RI.
This is not to say RI has necessarily reduced or ceased functioning in and of itself. Yet resting tonus becomes a competing force, and gradually over-powering RI.
At it’s simplest, the DSL Method is all about reducing Resting Tonus.
Primary Tools of DSL Edgework:
1. Let-Go Yoga (Low-Intensity, Physical/Mental Yoga)
Also known as “Conscious Stretching,” physical/mental yoga can be a highly effective tool for reducing C.E.M.&.N.T. and re-balancing muscle groups within the human bodymind. One available “yogic” objective, for motivated Clients or Patients, is to learn the skills of Feeling, Relaxing, Lengthening & Balancing their muscles.
In a properly designed and executed “stretch*,” the appropriate nerve endings — Golgi Tendon Organs (GTOs) — are stimulated, and the CNS spontaneously inhibits motor activity to the respective muscles on the same motor pathway.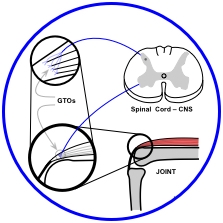
GTO Pathway
Using gentle stretching prevents activation of stretch reflexes, which can be triggered by extremely low amounts of tension or stretch, often below the threshold of awareness.
According to Arndt-Schultz Principle:
(SEE The Edge, A, Below) the gentle stretching action activates the parasympathetic nervous system. This is opposed to more aggressive yoga and exercise, which can inhibit parasympathetic activity, and even activate the sympathetic. Sympathetic activation is without doubt counter-productive to the desired Rest, Relaxation & Restoration, of the healing processes, as it tends to increase stress and tension in the bodymind.
On Yoga & Fitness Stretching Injuries: One reason I believe so many people are injured in stretching, yoga & fitness activities, is the stretch reflex can be so subtle as to be un-noticeable to the person. They are, therefore, often triggering muscle contractions that compress joints unknowingly. This is similar to an eccentric contraction, wherein the muscle can be lengthening, yet stays in a contracted state. An illusion of “flexibility” results, because the alpha system temporarily over-rides the gamma controlled, intrafusal fiber habit patterns. Yet when the alpha-controlled, conscious stretch activity stops, the gamma system takes back over, reinstating habitual, historical tension patterns, bringing the muscle back to a chronically shortened length.
The term “stretch” is not really a good one. It tends to imply elasticity, like a rubber band, spandex or pulling taffy. Many people approach “stretching” as if muscles and tendons were indeed elastic. The are not very much so. Muscle fibers are said to have the tensile strength half that of fine steel wire. Yet they can change length up to 150% of their length due to the “ratcheting” effect of the actin-myosin units (sarcomeres).
Fascia, including tendon, are widely stated to have a maximum of 6 to 7% extensibility. This provides a modicum of “shock absorber” effect for the musculo-fascial-tendinous unit. They have no detectable striated, contractile muscle fiber.
There are occasional locations of a few contractile, smooth muscle fibers, which have very little pulling power, and some researchers say these are anomalies resultant from injury. Therefore, there is no ability for them to actually contract in the fashion nor strength striated muscle fiber is capable of.
2. Hands-on, Yoga-based Bodywork
Often times, regular old stretching (ROS), or even Conscious Stretching, will not release C.E.M.&.N.T. if it has been allowed to progress too far over too much time. In such cases, manual applications of pressure (hands-on therapy) on the neuro-musculo-fascial units can achieve responses that inhibit C.E.M.&.N.T. and assist in returning it to more normal or neutral states.
This is a further opportunity to Feel, Relax, Lengthen & Balance muscles, but with a very different though related set of sensory inputs. Using both the stretch and the manual techniques, sometimes simultaneously, greatly expands the sensory-motor dimensions of the Client or Patient.
Why Manual Work is More Efficient: Medical research shows Golgi Tendon Organs (GTOs) to be far more sensitive to “internal” stretching than to “external” stretching. More specifically, the GTOs are more sensitive to stimulation from within the muscle belly than from the direction of the tendon.
The application utilized here is that an external stretching of the tissue (such as in a yoga pose) is achieved by pulling the ends of the muscle away form each other. The ends of the tendons move away from each other, activating GTOs, but in larger bundles of fibers.
Internal stretching can be achieved by applying manual pressure within the muscle belly itself. As the muscle fiber group moves as it is pressed, the tension is transmitted to the GTO at the musculo-tendinous junction. The more specific the pressure, on fewer numbers of fibers, the more precise is the stimulation to fewer GTOs.
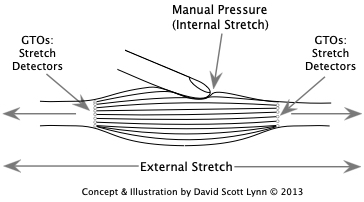
An overall stretch treats the muscle fibers more collectively, as a larger group. The more precise manual pressure addressing smaller groups of muscle fibers more individually, giving them more specific stimulation. Anyone who’s done much manual work in muscles has discovered that there are frequently very small areas within muscles far more sensitive, with much more rigid textures, then closely adjacent areas. If the neuromuscular discombobulation theory is correct, then these specific bundles of fibers need to be reset first, independently of their neighboring fibers.
Like Let-Go Yoga, an additional idea is to stimulate the parasympathetic system. Therefore, initially, very low-levels of manual pressure are applied to the tissues. This prevents clients from re-acting negatively and actually tightening up — via the stretch reflex or fear — when the objective is for them to let-go and relax.
3. BIO-Structural Balancing & DE-Compression — YogasAnalysis
The body is in a constant state of seeking structural homeostasis within the field of gravity and relative to internal pressures and forces (which can include emotional and mental factors at times). Just as metabolic homeostasis attempts to keep the body within certain ranges of function, so does the muscle system for structural integrity & responsiveness to the internal & external environment. This requires a constant readjusting of tension levels in muscles. Combine these factors with the accumulation of C.E.M.&.N.T. and you sometimes have quite a puzzle to work out.
Determining which muscle groups are not just “tight” but over-shortened relative to their counterparts is a critical element for discovering an “effecticient” (effective & efficient) return to a balanced state of being. Releasing muscle groups in the proper sequence — often working A-symmetrically for a period of time (which sometimes goes against “common wisdom”) — is very often the most effecticient way to bring a client or patient back to normal in the shortest amount of time with the least negative repercussions in the process.
Example: Psoas muscle is often responsible for many problems throughout the body. Releasing tension in the psoas often solves many problems. However, psoas is highly reactive to shortening of the hip extensors and abdominal / lumbar flexors. Psoas often relaxes and lengthens far more effecticiently when other relevant muscle groups are released first. In some cases, if the other muscles are not addressed first, the Client or Patient can have a significant increase of pain lasting for hours or days before the muscles return to their familiar, more compensated state.
There are people so out of balance that releasing their muscles — even though it is just relaxation — can actually throw them too far out of the “provisional balance” their body has been adaptively holding on to — sometimes for years or decades — to compensate for their deeper structural issues. This can cause significant amounts of pain and dysfunction, even if they are actually on their way back to health.
Other people have issues definitely made significantly worse by releasing muscles prematurely or out of proper sequence. Though not always perfect, proper structural analysis helps determine proper sequencing of the muscle release process, reducing likelihood of such negative reactions.
YogasAnalysis: is a system for creating, evaluating or prescribing yoga postures based on principles of BIO-Structural Balancing & Postural Evaluation. Structural Analysis tells you which muscles, or parts of muscles, are chronically over-shortened, exerting excess force on the structure. Through functional kinesiology, a yoga posture is then constructed that will best place the muscle in a slightly lengthened position, giving the Client or Patient the opportunity to discover the skills of Feeling, Relaxing, Lengthening & Balancing their muscles.
On the Lengthen/Strengthen Philosophy: It is often suggested that over-shortened muscles be stretched to lengthen them, and over-lengthened muscles be “strengthened” into a shorter position. In the early stages of therapy, I do not recommend this approach. Even thought the locked-long muscles are “stretched long,” they are still usually very tight and in need of rest & regeneration. They deserve a break today, and tomorrow, and for as long as necessary. Attempting to “strengthen” them prematurely has several potentially negative consequences.
Also, when in a stressed or trauma state, it is often very difficult for a Client or Patient to isolate muscles sufficiently, and they run the risk of contracting the very muscles we are trying to relax & lengthen.
While there will of course come a time they will have to be evaluated for SECC, we have never found the necessity for the Lengthen/Strengthen Strategy until the Client is well on their way back to structural balance. Yet, in many cases there allegedly lost strength returned without doing any strengthening at all. Their active insufficiency or exhaustion had been resolved, and their strength returned.
4. Tai Chi/Chi Kung-based Movement Therapy
In the spirit of parasympathetic stimulation, yet for people who are too impatient to do slow, long hold yoga postures, the gentle, partial range of motion of tai chi-based therapeutic movement is often ideal. It also serves as an excellent transition exercise for taking the principles of Let-Go Yoga into the realm of more overt movement, exercise & activity. The major key, however, is the slow, gentle stimulation of the parasympathetic system.
5. Internal & External Ergonomics
Much C.E.M.&.N.T. is caused by people placing their bodies in postures or actions more prone to development of imbalances between muscles, plus increased tension and stress. People are frequently able to RE-design their work stations as well as their home environment to either eliminate or at least reduce negative impacts on structural integrity. Sometimes, the simplest adjustments make the biggest differences.
6. Metabolic Support: Diet, Detox, Nutrition
[MORE COMING SOON]
From this point, the material is in more-or-less outline form, with many details filled in. Though not fully edited and fleshed out, it should provide a basic understanding of what we’re doing.
HOW to Work with a Neuromuscular/Myofascial Unit in a C.E.M.&.N.T. Condition
1. The EDGE: A.
The Primary Objective is to reduce the levels of C.E.M.&.N.T. and restore balance between muscle groups.
Parasympathetic Activation — Sympathetic De-Activation *
… defuse tension & stress patterns, internally heal resulting symptoms, dis-eases, syndromes, illnesses.
Arndt-Schultz Principle*:
• Weak Stimuli — tends to activate physiologic processes
• Moderate Stimuli — tends to favor physiologic processes
• Strong Stimuli — tends to inhibit physiological processes
• Very Strong Stimuli — tends to arrest physiological processes
“Physiologic Processes” refer to the Parasympathetic System
* Formerly known as the Arndt-Schultz Law, taught in medical schools in the early 20th Century.
~Taber’s Encyclopedic Medical Dictionary
When Rest, Relaxation & Regeneration, and Parasympathetic Activation are the primary goals, then Weak to Moderate Stimuli are the ideal levels of input to the nervous system. The more trauma and pathology a Client or Patient has, the closer to the Weak end of the spectrum the therapists should maintain.
The Health <==> Fitness Spectrum:
(Parasympathetic) Health < ==> Fitness (Sympathetic)
- Weak to Moderate Stimuli <==> Strong to Very Strong Stimuli
- Rest, Relaxation & Regeneration <==> Strength, Endurance, Cardio, Coordination
- Activates Physiological Processes <==> DE-Activates Physiological Processes
- Emphasizes Intrafusal Fibers <==> Emphasizes Extrafusal Fibers
Background, Non-Conscious Postural Balance <==> Overt, Sometimes Conscious, Volitional Action
In extreme cases — increased Stress, Injury and/or Trauma — REQUIRES ALL work be toward the Minimum Edge (lowest intensity possible). … Severe Trauma = “Severely” Light work.
Is all about Exploring and “Dissolving” the Limitations resulting from Physical & Mental — as well as Emotional* & Social — Resistance. … Resistance tends to show up in the form of C.E.M.&.N.T.
2. The EDGE: B.
How much Pressure to apply in manual medicine?
The Goldilocks Rule of Intensity:
Not Deep Enough — Just Right — Too Deep
Learning distinctions between intensity of sensation and actual pain.
When a therapist applies manual pressure, or a stretching technique is applied, the Client’s response is that the generated sensation is either … Too Deep, Not Deep Enough, or Just Right. .. If they are not sure, it is Too Deep.
Working with such requires a strategy of
Minimum (weak) Edge <==> Moderate Edge <==> Maximum (strong) Edge
Parasympathetic (weak) Activity <==> Sympathetic (strong) Activity
Maximum Health & Restoration <==> Maximum Strength/Endurance
YOGA:
SOFT: Restorative Yoga — Let Go Yoga < ==> Classical Yoga — Power Yoga :HARD
Martial Arts:
SOFT: Chi Kung — Tai Chi — Aikido — Kung Fu — Karate — Iron Fist — MMA (full contact) :HARD
Massage & Bodywork:
Lighter Manual Pressure <==> Deeper Manual Pressure
*Emotion: etymologically — e = to bring forth; motion = action. Therefore, emotion is that which brings forth action, which must include the muscles. … Muscle Cells are the Primary Vehicle of Self-Expression.
Emotion is at least as much in the muscles and nerves of the body — not to mention the neurotransmitters in the bloodstream — as it is in the mind, probably more so. The problem is, it’s mostly historical and usually forgotten conditioning based on fundamental and fully non-conscious reflex impulses. These either are, or tend to be, unconscious processes, and difficult to access unless trained in the art of bodymind introspection. And if they are accessed, it is probably only in an indirect way.
Body < == Emotion ==> Brain
Muscles/Sense Organs — Nerves — Feelings — Neurotransmitters — Memory — Thought
The emotional state is the Bridge between mind and body. It is not just an accessory or embellishment of life.
Ultimately, the Bridge is the unity of both mind AND body together, which are not really different things. When in The Zone, the distinction between them dissolves. This separation is, in many ways, illusionary and, if taken too far, creates anxiety, disassociation and dysfunction.
Having a Client Pay Attention to their Edges is a first step in making the unconscious conscious. Start by telling them to just report what they feel without trying to change it. Follow First Rule of not exacerbating a Client’s negative perspective or self-doubt. This leads to deeper surrender & relaxation, following a primary rule of meditation — to Be with What Is without exerting will power to change What Is.
Willpower is by definition a time-based process, therefore taking one out of the meditative moment of awareness.
Doing the above relaxes the mind and emotional states, activating internal healing processes. This is NOT pain avoidance. It is going up to it and taking a look at the pain or negative sensations, at their periphery, without triggering any negative reactions. Most of the desired changes occur as a natural result of the relaxation process, not by effort or force.
3. NeuroMuscular Relaxation — Turning OFF the Synapses
Stimulation of Golgi Tendon Organs within Client’s Current Edge:
Long-term, chronic tension and stress patterns are habitually held in place by modifications of the bio-chemical (and sometimes electrical) charge at the synapses. The synapses, via temporal and spatial summation, get, in layman’s terms, “stuck in the ON position.” … It can be difficult to turn them OFF, or they turn off, but turn right back on.
At one level, we are using manual pressure, range-of-motion, stretching or other relaxation techniques to inhibit the charge at the synapse. This is a neuromuscular or psycho-muscular PATTERN INTERRUPT. Give them opportunities to feel something different. Question is how long, and how often, is a particular input necessary to break the habitual stress or tension pattern?
Synaptic Modification — De-Facilitating the Bio-Chemical Synaptic Bath with steady, extended pressure via the muscle fibers to the Golgi Tendon Organs.
GTO’s Initiate Inhibitory Response at 2 levels:
Local Spinal Reflex Arcs ==> Long Tracts to Reticular Formation (Spinocerebellar Tracts)
Short-Term Local Tension Release ==> Long-Term Parasympathetic Response
Requires TIME to deactivate long-held neuromuscular and psychomuscular tension, stress and habit patterns. We’re waiting for the synapses to “Turn OFF.” Years or decades of bio-chemical modification at synapses is not easy to change.
A high trauma Client or Patient must be kept as close as possible to the absolute Minimum Edge, sometimes not even touching their body, for extended periods of time. Sometimes, just the thought of being touched can re-trigger trauma or fear patterns. They must adapt psycho-emotionally to the IDEA of being touched before actually being touched. (These are, of course, in extreme cases.) This can take some time, occasionally a LOT Of it.
The main reason most people in these conditions have never responded well to manual technique (massage, bodywork or joint manipulation) is it requires extended amounts of TIME — with minimal movement and pressure (even tiny motions can cause irritation) — to facilitate the needed release of stress & tension and parasympathetic activation. Such conditions require extremely slow, gentle applications of steady pressure, with little or no lateral movement, so as to not trigger stretch reflexes or other emergency response mechanisms of the body, which can trigger spasm or worse.
Some spasm occurs at such a minute and subtle level neither the client nor practitioner notices it. It is often these subtle stretch reflexes, the minute spasms, causing many of the negative reactions to therapy hours or days later.
Unfortunately, few practitioners of any modality, be it orthodox or alternative, are positioned logistically or economically to provide the necessary time needed for the needed level of care in more extreme cases. The amount of time required from one-on-one treatment is usually prohibitive from a time and money point-of-view.
4. Hilton’s Principle — Neuro-Fascial (Skin Rolling) Technique
Hilton’s Law: The nerve trunk (both sensory and motor) feeding a particular joint also feeds the muscles and skin over that joint.
Occasionally, the pain a Client or Patient feels to be very deep, is actually due to sensory nerve excitation from the skin and superficial fascia. Resolving this requires, for example, a “skin rolling” or very slow & gentle “pinching” technique (actually a squeeze and lift action of the skin & superficial fascia) to defuse the superficial irritations before working deeper.
It starts with a slow, steady, gentle, low pressure “pinch & hold” of the tissue with little or no movement, and NOT to anywhere near the point of pain, and holding relatively still till the tissue begins to soften, still respecting the Client’s preferred levels of The Edge, rather than the traditional rolling action in neuromuscular therapy, which can be quite painful. As the tissue loosens, then a soft, minimal rolling action can be used, increasing the lift of the skin away from the core of the body. This facilitates a defusing of hyper-irritated sensory nerves and pathways originating in the superficial layers, opening the doors for deeper work.
5. Evaluation/Reduction of RESTING TONUS:
A critically important distinction seldom made in any healing or fitness system (according to Taber’s Medical Dictionary):
TONE = A healthy state of the muscle
TONUS = Amount of bio-chemical or electrical charge moving through the nerve to and activating the muscle, organ or gland. Chronic activation of this charge leads to BodyMind Breakdowns.
Intrafusal Fibers, controlled by the gamma system and terminating in the reticular formation, are more difficult to de-facilitate on one’s own — with no direct connection to the conscious cerebral cortex.
Intrafusal Fiber activity is NOT detectable (at least, possibly, until recently ???) by EMG equipment, so assessment that a particular muscle is “weak” or “inactive” is often is without any real foundation. … There feels to be subtle differences between the “feel” of excess tonus in the intrafusal and the extrafusal fibers of a muscle.
It is my view that Excess Resting Tonus in Intrafusal Fibers is a primary issue for most postural imbalances in long-term, chronic tension issues.
Muscle “WEAKNESS” as a cause of most pain, posture & dysfunction problems is mostly a Myth-Conception. Just because a muscle is over-worked and exhausted is not a valid reason to call it fundamentally “weak.” Yet it is in a “weakened” state due to exhaustion, lost mechanical advantage, and active or lassie insufficiency.
In respect to posture, dysfunction and pain, in many if not most cases, the diagnosis of a “weak muscle” is a Health Care Tragedy of 20th Century.
Selective Tonus — Most Posture, Pain & Dysfunction issues are a result of chronically contracted, hardened and usually over-shortened, somewhat isolated, groups of muscle fibers, usually (but not always) deeper within a particular muscle.
Individual Muscles do not contract uniformly as a unit. Individual groups of muscle fibers within the muscle belly — usually initiating movement by fibers closest to the center-line of the joint — activate first. They are increasingly “covered up” or “surrounded” with layers of tension from other muscle fibers within the same muscle belly. The hypertonic fibers are “protected,” isolated and compensated for by their neighboring fibers. Therefore it takes more TIME to get deep enough to find them. Pressing too hard, too fast, causing the protecting tissues to react by tensing, often prevents finding and isolating the actual, deeper, target muscle fibers.
6. Davis’ Principle:
When the ends of a muscle fiber move towards each other, the tonus goes up. When the ends of the fibers move away from each other, the tonus goes down, causing them to “weaken.”*
Dorland’s 25th Edition
*Notice the quotes around the term “weaken.” The quotes imply “not exactly” or lend some doubt that the word is exactly descriptive. In that definition, the term “weaken”should actually be something like “fires less frequently” and/or “fewer motor units are firing.”
Davis’ Principle is the principle by which Nature does not allow for a slack muscle in the body; yet muscles, while maintaining proper length at all times, must also be ready to lengthen instantaneously, allowing for quick, precise, fluidly stable movement. This is, for example, critical for responding to or escaping danger.
Increased resting tonus inhibits the ability and responsiveness of muscles to change or respond along with changing conditions.
This is why, if you are going to REALLY release a muscle, you must get to ALL the fibers in a shortened position. Otherwise, the fibers that did lengthen will tend to return to the length (shortening back down) of the most shortened adjacent muscle or fiber group. You must also release the fibers in other muscles that are shortened as well. The shortest fibers will control the span of the joint, even if to adjacent to the target fibers.
Synergistic Contractors, though not themselves traumatized nor initiating the original problem, will short to take up any excess slack in the muscles. The more stress, trauma, or injury to the local area, the more aggressively these synergistic fibers will “participate” in the protective action.
Reciprocal Inhibition (RI) is interfered with by this increase of resting tonus. RI is next to useless as a tool of healing modality when people get to the severe, chronic tension & stress states.
7. Yoga versus Manual Pressure Techniques:
Yoga and Manual BodyWork tend to stimulate and affect different nerve endings, therefore sending different types of signals into the CNS, producing different though related neuromuscular effects.
Although there is significant overlap, yoga and stretching tend to stimulate the more proprioceptive and structurally related nerve endings; i.e., Golgi Tendon Organs and muscle spindles. Manual massage & bodywork additionally tend to affect the pressure sensitive nerves in the skin and superficial fascia, as well as providing a stretching action. Deeper cross-fiber accesses both, but not as efficiently as steady pressure in specific places for extended time.
Renshaw’s Cells: MY Current Personal Theory — Not Yet 100% Sure About
Both approaches affect Renshaw’s Corpuscles, which, with appropriate stimulation, send an inhibitory signal to the motor units in the nearby region of the originating sensory input. Treatment must not trigger a stretch reflex or other negative response that would over-ride the action of Renshaw’s Corpuscles.
Structural Analysis: Determining WHERE to Work:
Tension & Stress
/
1. Localized Reaction to Trauma or Injury
\
Postural Misuse
/
2. Structurally Transmitted — Stress or Trauma
\
Repetitive Action
/
3. Neuralgic Transmission — Nerve Entrapment
\
Stress or Trauma
/
4. Antalgic* Postural Reaction — Nerve Entrapment
5. Generalized Compression — No Specific Postural Deviation from Centerline
\
Repetitive Action
Neuralgic Transmission, or its more subtle precursors, is the Wild Card
Basic Principle of Postural Evaluation — Structural Homeostasis
Determine the shorter & longer angles at each joint segment.
The Shorter Angle is location of the Adaptively Shortened or Locked Short muscle. This is the muscle(s) to treat.
The Long Angle (opposite side) is location of the Adaptively Lengthened or Locked Long muscle. This is usually the pain site. Except in certain circumstances, we do NOT treat these muscles until the body has moved substantially back toward structural balance.
Antalgic posture reacting to localized trauma, pain, etc. reverses the pattern. This is the hardest to detect via visual analysis.
Helps to get good at observing the action of physical forces and gravity on, and reaction of, the body.
EXAMPLES:
Weakened thumb result of over-shortened abdominal and chest muscles acting on the brachial plexus at clavicle.
Tension and Pain in neck and shoulders result of over-shortened lumbar flexor (abdominal) and hip extensor (hamstrings and gluteals) muscles that are posteriorly tucking the pelvis, flattening lumbar curve, depressing the rib cage, pulling neck and head down and forward.
Basic Structural Model of Posture
Primary Force lifting the body up is Hydrostatic Pressure throughout body and at joints.
The Fascia creates the “bags” that contain water.
The Bones keep the ends of the water bags from getting too close to each other, maintaining length (height) of body.
Primary Force holding the body upright is Gravity pulling equally on all sides of the body.
The Muscles manage the relationship between the bones, the water, and the gravity.
The Basic Postural Distorting Force is Excessively Short Muscles which overpower & condense the buoyant & expansive force of hydrostatic pressure.
SPECIFIC MUSCLE ACTIONS:
Primary Muscle for maintaining upright orientation of upper torso is Transversus Abdominus compressing the water of the abdomen, like a girdle.
It also is primary actor in creating a proper DE-compressive lordosis. In modern society, true “excess lordosis” seems comparatively rare.
It is an error to attribute “strong” elector spinae (back muscles) with unloaded vertical posture. Spinal Erectors only need to recruit when weight is applied anteriorly or laterally of the vertical center.
The Lateral Obliques maintain side to side orientation of rib cage while Quadratus Lumborum stabilizes vertebral orientation.
Psoas muscle is NOT a primary stabilizer of spine in normal, relaxed, unloaded, upright posture. It gets recruited by lumbar flexion from Abdominals and posterior pelvic rotation by hip extensors.
Excess contraction & softening of Psoas Major is a primary cause of spinal disc compression, herniation and rupture. Deep fibers of Psoas Major pull on and irritate lumbo-sacral ligaments via their anterior attachments.
A Primary Muscle for maintaining anterior/posterior Pelvic orientation is posterior portion of Abductor Magnus which stabilizes pelvis regardless of knee action and angle.
Primary Muscle for side to side orientation of Pelvis are Gluteus Minimus and probably Medius.
Thank You Very Much for taking the time to review this summary
of the physiology of the DSL Method of Yoga & Bodywork.
Please e-mail me with any questions, comments, concerns or suggestions at:
admin (at) davidscottlynn (dot) com
Take Care,
David Scott Lynn
- Only YOU Can Prevent Yoga Injuries! - February 6, 2015
- Does Psoas Cause Lordosis? - June 11, 2014
- MyoFascial Facts & Fallacies - June 7, 2014
Comments
Summary for Physicians & Therapists — No Comments
HTML tags allowed in your comment: <a href="" title=""> <abbr title=""> <acronym title=""> <b> <blockquote cite=""> <cite> <code> <del datetime=""> <em> <i> <q cite=""> <s> <strike> <strong>